![]()
|
|
DEMENTIA AWARENESSCERTIFICATE COURSE
UNIT THREE |
|
|
CARE: THEORY AND PRACTICE |
Introduction
In achieving this learning outcome you will explore your own perceptions and experiences of working with people with dementia, and comparing these to research that has specifically addressed the nature of person-centred care. This will involve, firstly, exploring what is meant by person-centred care, and its importance within dementia care. Then, there is a need to consider the elements of person-centred care and how these can be realised in practice. Finally, means of implementing person-centred care will be related not just to the person with dementia; consideration of the carers (both formal and informal) will also be discussed with reference to relationships.
|
|
ACTIVITY 3.1: QUESTION |
As an introductory activity to get us thinking about the nature of care, imagine you have been admitted to hospital.
How would you want to be treated?
How would you not want to be treated?
|
|
What is Person-Centred Care? |
Over a decade ago, Kitson (1996:1649) asked the pertinent question:
“What is care? And do we value it?”
The concept of care has been much discussed in print over the years. Since Travelbee (1963), there has been a plethora of articles on what constitutes care published in the 1980s (for example, Gadow, 1980; Leininger, 1980; Bevis, 1981; Griffin, 1983; Watson, 1985; Dunlop, 1986; Green-Hemandez, 1988; Homer, 1988), the 1990s (for example, Koldjeski, 1990; Roach, 1991; Swanson, 1993; Eriksson, 1994) and still the topic is covered (for example, Schoenhofer, 2002a; 2002b; Fredriksson & Eriksson, 2003; Maldonado et al, 2003; Schmidt, 2003; Turkel, 2003; Watson & Eoster, 2003; Boykin et al, 2004; Karlsson et al, 2004; Boykin et al, 2005; Mantesso, 2005; Touhy et al, 2005; and Wolf et al, 2005).
Yet, as Paley (2001:188) notes, these writers are:
“describers on the same treadmill, rather than the ultimate definers”
By this he means that the outcome of all the work is still vague. Indeed, he cites Foucault’s (1970) words as summing up the case that the literature is:
“plethoric and yet absolutely poverty stricken” (Paley 2001:30)
Why is this? Referring to Activity 3.1, you know doubt could state clearly how you would like to be treated and cared for if in hospital. Indeed, if you were to ask anyone, all would be able to state what constitutes “good” care and what constitutes “bad” care for them. Yet, the literature appears devoid of clarity on this matter.
|
|
ACTIVITY 3.2: QUESTION |
Conduct a literature review to answer the following question: “What is care?”
Caring has come to be perceived in different ways. For example, it could refer to:
Aspects of the organisation (the “caring” organisation)
Tasks to be done (“care” given)
Behaviours (the act of “caring”)
The nurse effect and characteristics (nurse as being “caring”)
Patient perceptions (being “cared” for)
Student nurse perceptions (giving “care” under supervision)
Perceived outcomes of the caring task (successful “care”)
As such, Mackintosh (2000:326) noted that the:
“relationship of caring and nursing is a highly complex nebulous arrangement”
In her review of the literature, Sumner (2006) noted that part of the reason for this is because of the different perceptions of care, and the frequently limiting nature of the discussion that focuses upon either the nurse perception of care given, or the patient’s perception of care received, without a clear acknowledgement that this is a two-way process. In her concept analysis, she differentiates three aspects to be considered in relation to care:
The nurse
The patient
The environment
Sumner (2006:13) defines caring in nursing as:
“communicative action, framed by the universal conditional ought of respect for all human life, encompassing the spectrum of human experience, and is manifest in the verbal and nonverbal discourse between two equal and vulnerable human beings”
This definition is useful because it makes some interesting points about caring within the caring relationship that are sometimes overlooked. Firstly, it acknowledges that caring has a goal (it is a form of communication). Secondly, it states that it is based on certain values and beliefs (respect for others). Finally, it occurs within a relationship of equality (two equal and vulnerable human beings).
|
|
ACTIVITY 3.3: QUESTION |
Considering each of these three elements of caring, reflect on your own practice and write in what ways they are an accurate depiction of your relationship with your clients:
The goal of caring?
The value-base of caring?
The equality of the caring relationship?
|
|
Person-Centred Care |
If “care” is a difficult concept to delineate, then the various terms we find in the literature pertaining to “person-centred” (Kitwood 1997), “patient-centred” (Gerteis et al 1993), “person focused” (Cheston and Bender (1999) and “client-centred” (RNAO 2002) equally provide a “murky” (Morse 1995:37) understanding.
|
|
ACTIVITY 3.4: QUESTION |
What does person-centred care mean to you?
In their attempt to delineate the meaning of what they refer to as “patient-centred care”, Gerteis et al (1993) note the following factors:
Respect for patients’ values, preferences, and expressed needs
Coordination and integration of care
Information, communication, and education
Physical comfort
Emotional support and alleviation of fear and anxiety
Involvement of family and friends
Transition and continuity
Within a dementia care context, it is about seeing the person with dementia and not the person with dementia. It is thus about “putting the person first” (Kitwood 1997).
|
|
ACTIVITY 3.5: QUESTION |
The first point of patient-centred care according to Gerteis et al (1993) was:
Respect for patients’ values, preferences, and expressed needs
Consider your work with people with dementia.
How do you know the values, preferences and expressed needs of your clients?
In what ways do you show them that you respect them?
Although the word “person” has been consistently used over time, its meaning within a Western context has changed (Cassel 1982, Kitwood 1990). Its understanding in relation to the brain has led to some debatable conclusions. For example, a person is often seen in terms of the ability to be an agent, that is,
“a being that has the ability to pursue chosen purposes” (Pattinson 2006:548)
However, if a person experiences brain damage, they become a “non-agent”. This has led to such views as people with dementia ceasing to become “people” (Dworkin 1993). Often, the literature refers to personhood as consisting of various attributes that constitute their humanity (McCormack 2004). For example, Cassel (1982) states that the attributes of being a person are:
Having a past
Having a cultural background
Having roles
Having relationships with others
Having a political dimension
Doing things including action and creation
Engaging in regular behaviours
Having a body
Having a secret life
Having a perceived future
Having a transcendent or spiritual dimension
The problem with devising such lists of attributes is that they are values-based and, upon reflection, can include as well as exclude. For example, Post (1995) talks about the dangers of “hypercognition”, that is, the prizing of cognition above anything else. This is of course pertinent to people with dementia because of their difficulties with cognition that lead, once again, to them being excluded from the label “person”.
One approach to conceptualising person-centred care with particular reference to dementia is the so-called VIPS model (Brooker 2007). This model, based on a literature review that Brooker (2004) conducted, conceptualises person-centred care as incorporating four distinct but interrelated elements:
V Valuing the person
I an Individualised approach (which recognises a person’s uniqueness)
P understanding the world from the Perspective of the service user
S promoting a positive Social psychological milieu (where people can experience well-being)
|
|
ACTIVITY 3.6: QUESTION |
Consider the VIPS model as proposed by Brooker (2007).
In what ways does your practice align itself to these four aspects of person-centred care?
In what ways can it address these four aspects?
In Unit Two, we considered Kitwood’s (1997) conceptualising of dementia as being more than a neurological impairment. He considered aspects of malignant social psychology that also affect the person with dementia. In his book, he cites the following case of a formal carer working on a dementia care unit who after completing their task, went to see what else needed doing:
This was a large room with four beds, four chairs and four commodes; it was home to four ladies with dementia. As I entered, the door was wide open; all four ladies were sitting on their commodes, and the smell of faeces permeated the air. There were no curtains or partitions to screen the ladies from each other or anyone else walking past. My colleagues Sandra and Mary were feeding two of the ladies, and talking about the night out they had just spent together. Sandra was feeding Mrs. T. As soon as there appeared a little room in her mouth, more food was inserted. Her cheeks were bulging with food she hadn’t had a chance to swallow. Mrs. T started to gag; food began to spill from her mouth; then she coughed and sprayed Sandra with half-chewed food. Sandra proceeded to clean herself up, while leaving Mrs. T with food debris all over her clothes and exposed thighs. (Kitwood 1997:45)
|
|
ACTIVITY 3.7: QUESTION |
Reflect on the account you just read from Kitwood (1997).
In what ways were the people with dementia deprived of their personhood?
Why would such practices exist?
Kitwood (1997) listed seventeen ways in which we can depersonalise the person with dementia. In the above scenario, we see several of them illustrated.
|
Box 3.1: Malignant Social Psychology |
|
Treachery: using deception to distract/manipulate/force compliance Disempowerment: preventing/failing to help the PwD from completing a task Infantilisation: treating a PwD very patronisingly Intimidation: use of threats/power to induce fear Labelling: interacting with a label (behaviour/condition) rather than the person Stigmatisation: treating a PwD as a diseased object/alien/outcast Outpacing: going too fast for the PwD to understand/act Invalidation: failure to acknowledge subjective reality/feelings of the PwD Banishment: excluding the PwD physically or psychologically Objectification: treating PwD as an object rather than a sentient being Ignoring: carrying on as if PwD were not present Imposition: forcing PwD to do something without a choice Withholding: refusing to give attention/meet an expressed need Accusation: blaming PwD for something they cannot help doing Disruption: breaking into the PwD’s frame of reference Mockery: making fun of the PwD’s actions Disparagement: giving the PwD messages that damage their self esteem |
Your answers to Activity 3.7 may have noted examples of some of these aspects of malignant social psychology, what Sabat (2001) refers to as “malignant positioning”. For example, the people with dementia were treated as objects to be fed and toileted, without considering them to be sentient beings with feelings. They were ignored as the staff spoke to each other, not paying attention to the pooling of food in the lady’s mouth and, when she eventually spat it out, they considered their own needs and did nothing to clean and tidy up the person with dementia.
|
|
ACTIVITY 3.8: QUESTION |
Consider a typical situation with regard to your work with people with dementia.
Reflect on your care in relation to the seventeen aspects of malignant social psychology listed by Kitwood (1997)
In what ways do you or your colleagues exemplify some of these factors?
In what ways could you or your colleagues counter some of these factors?
Whilst the literature stresses the importance of seeing the person not the disease (Kitwood 1997), valuing them (Brooker 2006) and treating them with dignity and respect (Dennis and Morgan 2008), it is clear that this is not always the reality. Kitwood and Benson (1995) relate this to the differences inherent in the “old” culture and the “new” culture. This distinction is illustrated by Dewing (2007) when she compares two nurses, Tom and Clare. Tom believes that people “suffering” with dementia are vulnerable and need to be protected (that is, a paternalistic attitude). He also holds the belief that they are unable to make their own decisions (that is, they are non-agents). Clare, by contrast, believes that people with dementia are “survivors” who need to have as much freedom as possible (that is, a person-centred attitude). She also believes that they can make decisions for themselves, even when they are well into the dementing process (that is, they are agents).
|
|
ACTIVITY 3.9: QUESTION |
Considering the two nurses Tom and Clare, how do you think they would address the following:
|
|
Tom’s Actions |
Claire’s Actions |
|
Carrying out an Assessment
|
|
|
|
Definition of Risk
|
|
|
|
Actions in relation to Mobilising
|
|
|
|
Personal hygiene
|
|
|
|
When discussing care
|
|
|
|
When supervising students |
|
|
Upon reflection, what are the implications for the person with dementia with the two approaches exemplified by Tom and Claire?
The attitudes and belief of the nurse can have a profound effect upon the whole process of care given to the person with dementia. If dementia is perceived as solely a neurological condition and, at the present time, is incurable, then a paternalistic attitude will dominate and the person with dementia will simply be seen as a person (at best) or an object (at worst) who requires caring for. If, on the other hand, dementia is perceived as having a psychosocial component and that it does not mean the destruction of the person (for example, a “living death”), then care can be conceptualised as a mutual process between equals. Dewing (2007:43) notes the following outcomes of the differing approaches:
|
Table 3.1 |
||
|
|
Tom’s Actions |
Claire’s Actions |
|
Assessment
|
PwD not consulted for information. Information gained from other sources (e.g. notes, carer) |
Actively engages the PwD in the assessment process and seeks consent wherever possible |
|
Risk assessment
|
Always scores as high risk and therefore seeks to ensure safe environment |
Uses risk assessment as guide, along with information from home to make decisions |
|
Mobilising
|
Ensures escort when mobilising, and returns the PwD to seat/bed to ensure their safety |
Allows space for PwD to mobilise freely in a safe environment |
|
Personal hygiene
|
Decides for the PwD when it is time, and does it for them if not able to do task at same rate as themselves |
Negotiates time with PwD and assists only when needed |
|
When discussing care
|
Uses language that stresses the PwD as “hard work” and focuses on their inabilities |
Uses language that shows dignity and respect for the PwD and focuses on their strengths |
|
When supervising students |
Gives a negative picture of dementia (eg crisis management and harm minimisation). Role models provide poor appreciation of PwD’s subjective reality |
Gives a positive picture of dementia (eg promoting autonomy and independence). Role models provide excellent appreciation of PwD’s subjective reality |
From the above, it is quite clear that care for the person with dementia will only change if the next generation of carers witnesses a more positive approach by its superiors. Person-centred care will only become a reality if this occurs.
The processes of malignant social psychology are quite clearly damaging to the person with dementia. Kuhn and Verity (2002) proposed the following means by which these processes could be countered:
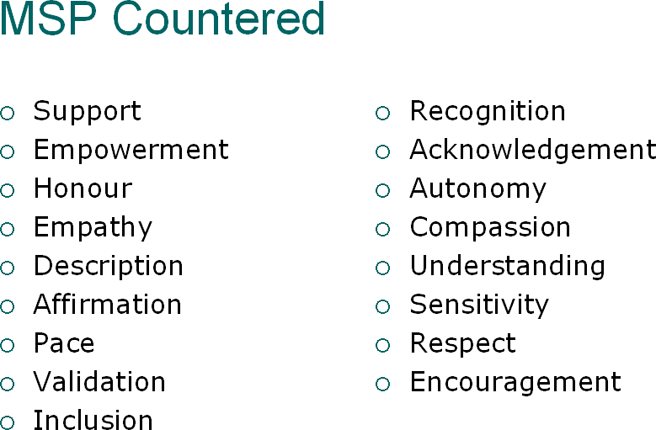
Figure 3.1: MSP Countered
These may reflect some of the ways you outlined in your answers to Activity 3.8 above.
|
|
Relational Care |
In the last decade there has been a move away from person-centred care towards a more relational-care model. At the time Packer (2003) was talking about “turning rhetoric into reality” with regard to person-centred care, Nolan et al (2004) was talking about going “beyond person-centred care” and proposing a “new vision” for working with older people. Whilst the National Service Framework for Older People (DH 2001) is based on two main principles:
Promoting person-centred care
Eradicating age discrimination
some have noted limitations of this approach, even doubting if person-centred care can ever become a reality (Packer 2000). For example, person-centred care focuses on two concepts (Hanford et al 1999):
Autonomy
Independence
|
|
ACTIVITY 3.10: QUESTION |
Reflect for a moment on the two concepts:
Autonomy
Independence
What do these words mean to you?
Is it possible for a person with dementia to experience these when they come into contact with health and social care services?
Autonomy is derived from two Greek words (auto + nomos) and, literally, means to give onself one’s own law. It refers to the ability of a person to make an informed and uncoerced decision. In ethics, it refers to the capacity of the individual to make moral choices by processes of self-determination (Kant 2003). Within medical ethics, autonomy is central to the concept of informed consent (Beauchamp and Childress (2008). However, as we have seen, the person with dementia is frequently viewed as a “non-agent” and, therefore, is not autonomous.
Linked to autonomy is the notion of independence. The idea that a person maintains their independence when in a caring relationship has been questioned by some (McCormack 2001). The issue is one of power relationships within the health and social care settings (Neal 2003). This is exemplified by Solzhenitsyn (1971:450) when he describes Dontsava, a doctor, telling a colleague that she has become ill. He writes:
“Yet having confessed to being ill, was like having confessed to a crime: immediately they had lost the key to equality they once possessed. By her confession she had excluded herself from the noble estate of medical men and transferred herself to the tax-paying, dependent estate of patients”
McCormack (2001) notes that the notion that older people within a healthcare context are autonomous and independent is “untenable”. In Activity 3.9 you reflected on concepts of autonomy and independence and considered whether or not they were possible for a person with dementia to experience once they come into contact with services. Goldsmith (1996) argues that this is because services do not allow the person with dementia to have a voice. Indeed, care is seen to be similar to that commented upon several decades ago, when Whitehead (1969:23-24) noted:
“Patients were herded together in old, bleak, neglected buildings with large, dark wards, closely placed rows of beds, little furniture and frightening inactivity. Multiple regulations curtail the patients’ freedoms and reduce their contact with the outside world. They may be confined to the ward and allowed out only in large supervised groups. Privacy, usually valued by the elderly, is often non-existent. Bathing is supervised and may take place in a communal bathroom. Visiting is restricted to a few hours a week and children are often prohibited. To visit some wards for the elderly is to visit the annex to the mortuary. Rows of old people lie in bed with legs bent and muscles wasted by lack of use, eyes dull and vacant, waiting to die”
In such an environment, it is difficult to envisage a person with dementia being autonomous and independent. Yet, has much changed since Whitehead (1969 wrote his words?
Are people with dementia nursed in institutionalised care settings?
Are people with dementia allocated bedrooms that require them to sleep in a group setting with little privacy?
Are people with dementia engaged with their local community or excluded?
Are people with dementia given privacy when bathed? Do they have their own bathroom facilities or do they share these with others?
Are people with dementia cared for in settings that have defined visiting hours?
Are people with dementia actively engaged in physical activity?
With the acknowledgement of the difficulties inherent in providing person-centred care that promotes autonomy and independence, the debate has moved to considering the applicability of relational care. According to Suchman (2006:40):
“Relationship-centred care is a clinical philosophy that stresses partnership, careful attention to relational processes, shared decision-making, and self-awareness”
|
|
ACTIVITY 3.11: QUESTION |
This activity will give you the opportunity to explore the components of relationship-centred care and reflect on their relevance to your own practice.
Access the following article by Beach and her colleagues (2006)
http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1484841&blobtype=pdf
Reflect on the four principles of relationship-centred care that they outline in relation to your own work.
Principle 1: Relationships in health care ought to include dimensions of personhood as well as roles
What does this principle mean to you?
In what ways do you act in an “authentic” manner with the person with dementia?
Principle 2: Affect and emotion are important components of relationships in health care
What does this principle mean to you?
In what ways do you display “emotional presence” with your clients/patients?
Principle 3: All healthcare relationships occur in the context of reciprocal influence
What does this principle mean to you?
In what ways do you “grow” as a result of working with people with dementia?
Principle 4: Relationship-centred care has a moral foundation
What does this principle mean to you?
In what ways do you act “genuinely” in your relationships with people with dementia rather than act out of your role?
Beach et al (2006) outlined four principles that constitute relationship-centred care. These principles highlight:
All illness occurs within a relational context
The centrality of the quality of the relationship in healthcare
The need for all participants in care to appreciate the importance of these relationships
As such, it goes beyond the simple dyadic model of care that just sees the therapeutic relationship as consisting of:
|
Carer |
|
Person with Dementia |
Rather, it sees the relationships of all participants within the context of the organisational:
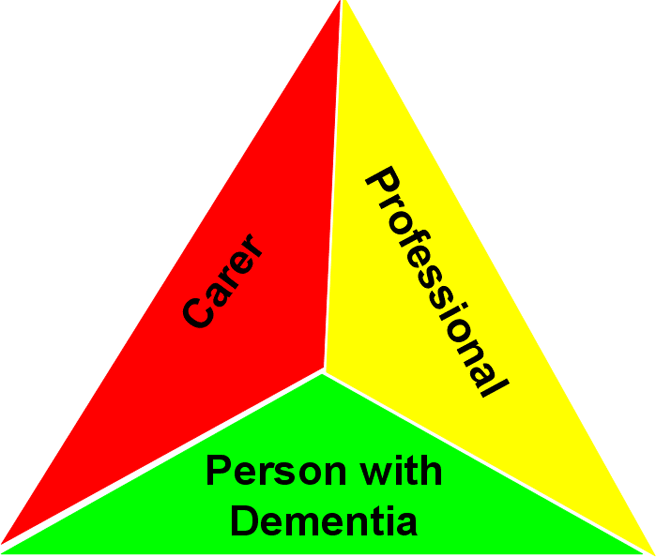
Figure 3.2: Triadic Relationships
Nolan et al (2001; 2004) outlined their “Senses Framework” to conceptualise all of these aspects of relationship-centred care. They stress that all participants should experience these “senses” in order for good quality care to be achieved. They define six “senses”:
The sense of security: to feel safe within the relationship
The sense of belonging: to feel that you are a part of things
The sense of continuity: to experience consistency in care
The sense of purpose: to have personally valuable goal(s)
The sense of achievement: to experience progress towards these goals
The sense of significance: to feel that you matter
|
Table 3.2 The Senses Framework (Nolan et al 2004:50) |
||
|
For Person |
For Carer |
For Staff |
|
Sense of Security |
||
|
Attention to essential physiological and psychological needs, to feel safe and free from threat, harm, pain and discomfort. To receive competent and sensitive care. |
To feel confident in knowledge and ability to provide good care (to do caring well – Schumacher et al 1998) without detriment to personal well-being. To have adequate support networks and timely help when required. To be able to relinquish care when appropriate. |
To feel free from physical threat, rebuke or censure. To have secure conditions of employment. To have the emotional demands of work recognized and to work within a supportive but challenging culture. |
|
Sense of Belonging |
||
|
Opportunities to maintain and/or form meaningful and reciprocal relationships, to feel part of a community or group as desired. |
To be able to maintain/ improve valued relationships, to be able to confide in trusted individuals to feel that you’re not ‘in this alone’. |
To feel part of a team with a recognized and valued contribution, to belong to a peer group, a community of gerontological practitioners. |
|
Sense of Continuity |
||
|
Recognition and value of personal biography; skilful use of knowledge of the past to help contextualize present and future. Seamless, consistent care delivered within an established relationship by known people. |
To maintain shared pleasures/pursuits with the care recipient. To be able to provide competent standards of care, whether delivered by self or others, to ensure that personal standards of care are maintained by others, to maintain involvement in care across care environments as desired/appropriate. |
Positive experience of work with older people from an early stage of career, exposure to good role models and environments of care. Expectations and standards of care communicated clearly and consistently. |
|
Sense of Purpose |
||
|
Opportunities to engage in purposeful activity facilitating the constructive passage of time, to be able to identify and pursue goals and challenges, to exercise discretionary choice. |
To maintain the dignity and integrity, well-being and ‘personhood’ of the care recipient, to pursue (re)constructive/reciprocal care (Nolan et al., 1996). |
To have a sense of therapeutic direction, a clear set of goals to which to aspire. |
|
Sense of Achievement |
||
|
Opportunities to meet meaningful and valued goals, to feel satisfied with one’s efforts, to make a recognized and valued contribution, to make progress towards therapeutic goals as appropriate. |
To feel that you have provided the best possible care, to know you’ve ‘done your best’, to meet challenges successfully, to develop new skills and abilities. |
To be able to provide good care, to feel satisfied with one’s efforts, to contribute towards therapeutic goals as appropriate, to use skills and ability to the full. |
|
Sense of Significance |
||
|
To feel recognized and valued as a person of worth, that one’s actions and existence are of importance, that you ‘matter’. |
To feel that one’s caring efforts are valued and appreciated, to experience an enhanced sense of self. |
To feel that gerontological practice is valued and important, that your work and efforts ‘matter’. |
|
|
ACTIVITY 3.12: QUESTION |
Consider the “senses” framework in terms of your own practice.
Reflect on how you would facilitate all participants in the relationship to experience each of these six senses:
Sense of security:
The person with dementia:
The family carer:
Yourself:
Sense of belonging:
The person with dementia:
The family carer:
Yourself:
Sense of continuity:
The person with dementia:
The family carer:
Yourself:
Sense of purpose:
The person with dementia:
The family carer:
Yourself:
Sense of achievement:
The person with dementia:
The family carer:
Yourself:
Sense of significance:
The person with dementia:
The family carer:
Yourself:
Such a framework is consistent with the relationship-centred care concept in that it acknowledges the centrality of the relationship. It also offers a useful means of considering all participants in care (the person, the family carer and the professional carer). Finally, the actual senses themselves offer a means by which the person is not forgotten in the process of care.
|
|
The Caring Environment: The “New Culture” of Care |
So far we have explored the nature of person-centred care and the important contribution that relationship-centred care offers in terms of considering all participants in the therapeutic relationship. However, all of this occurs within an organisational context that needs to be explored. The National Service Framework for Older People (DH 2001) proposes eight standards that should be met in terms of caring for older people. As stated previously, they are all founded on two central principles:
Age discrimination
Person-centred care
With regard to the standard pertaining to person-centred care, it states that its aim is to:
“ensure that older people are treated as individuals and that they receive appropriate and timely packages of care which meet their needs as individuals, regardless of health and social services boundaries”
It goes on to state that this to be achieved by:
The single assessment process
Integrated commissioning arrangements
Integrated commissioning of services
Single Assessment Process
The single assessment process consists of various domains that need to be assessed for:
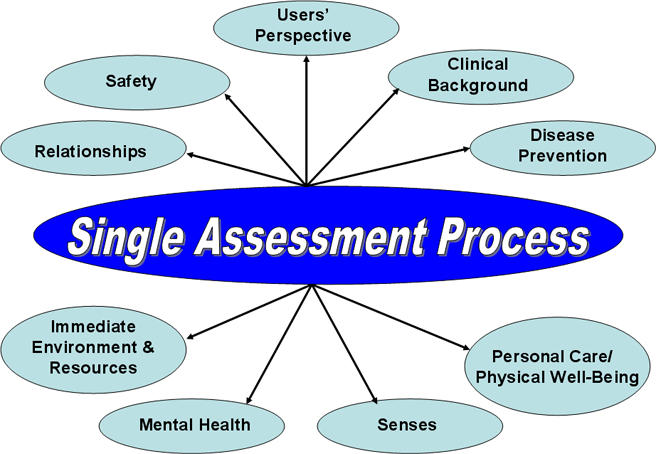
Figure 3.3: Single Assessment Process
|
|
ACTIVITY 3.13: QUESTION |
Consider each of these areas of need that are part of the Single Assessment Process.
(Details can be found in the NSF-OP (DH 2001: 32-33) document available online at:
http://www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/DH_4003066
In the assessments that you perform, are there any areas that are not covered that are referred to in the single assessment process?
How do you assess each of the areas of need pertinent to your area of practice?
The guidance for an accredited assessment scale outlines the following fourteen criteria (DH 2003):
The wording and structure of the tool should facilitate a person-centred conversation suitable for older people and professionals alike
The tool should make the contribution of older people to their assessment explicit
The tool should keep older people’s views, wishes, strengths and abilities to the fore
The tool should make the impact of older people’s environments, relationships and other factors on their needs explicit
The tool should be presented and designed to support professional judgement
The tool should help professionals to link different parts of the assessment, evaluate risks, and refer on to other agencies
The tool should take fair account of age, gender, race, disability and other factors that may have a bearing on needs and care plans
The tool should adequately cover the domains/sub-domains of the Single Assessment Process
The tool should be suitable for use by a range of health and social care professionals
Manuals and guidance should giver clear instructions on how the tool should be used, by whom and when
The tool should not be contractually bound to the provider of a single software solution
The tool should be capable of producing information for the Single Assessment Summary
The tool should use national standard data-sets where appropriate as they are, and become, available
The tool should satisfy statutory requirements with respect to consent and confidentiality, including the Human Rights Act 1998.
|
|
ACTIVITY 3.14: QUESTION |
Reflecting on the criteria for an acceptable assessment tool in relation to the single assessment process (outlined above), consider the tools you utilise and evaluate them in relation to these criteria.
Integrated Commissioning
The recently published National Dementia Strategy (DH 2009) outlines its vision for dementia services that include:
Improving the diagnosis process by changing public and professional attitudes
Providing a specifically commissioned service to aid in the early diagnosis and treatment of dementia for all
Good quality care provision for both the person with dementia and their carers from diagnosis to end-of-life care, in both community and hospital settings
The National Dementia Strategy (DH 2009: 22) has also provided a “vision” for its service development by means of a care pathway:
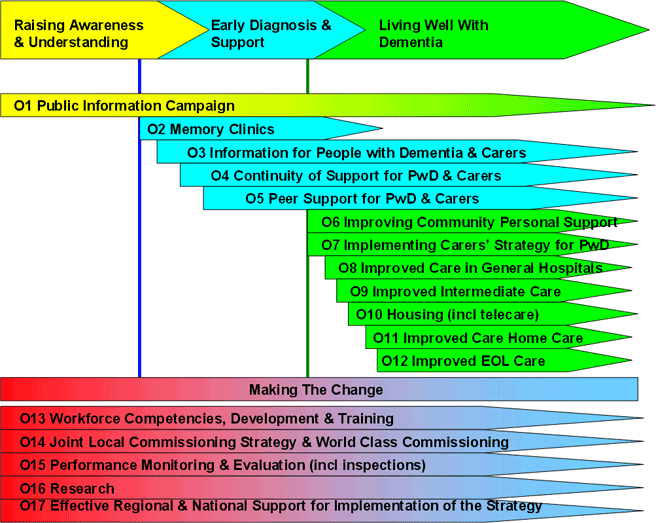
Figure 3.4: National Dementia Strategy
|
|
ACTIVITY 3.15: QUESTION |
Consider the service provision for dementia care in your area. In what ways does it mirror the vision proposed in the National Dementia Strategy?
Considering the three points that define this vision (listed above), reflect on your current practice and analyse it in light of these.
It is quite clear that for a service to be a quality service, then values need to be considered. They are the foundation for any debate about quality because, as Cox (2001) notes, they:
Affect how quality is defined
Affect how quality is interpreted
Affect how quality is implemented
In her earlier work, Cox (1998) outlined five core values of a dementia care service. Such a service:
Maximises personal control
Enables choice
Respects dignity
Preserves continuity (links past, present and future for the person with dementia in the context of service provision, living environment and care processes)
Promotes equality
Gaster (1995) has proposed a model for developing a quality service that highlights both the values-based foundation of the service and how these relate to strategic processes and outcomes. If the vision is to provide a service that empowers the person with dementia, treats them with dignity and respect, offers them real choices and is a seamless service, then the actual service will reflect these values. Just as we considered the implications of our own values by reflecting on the two nurses, Tom and Clare (Activity 3.9 above), so too, these are reflected at an organisational level.
Kitwood (1995) advocated that there was a need for a change of culture to take place within organisations in order to facilitate improvements in the quality of care for people with dementia. A similar cultural shift is needed in order to realise the vision described in the National Dementia Strategy (DH 2009).
|
Table 3.3 The Cultures of Care (KItwood 1997) |
|
|
Old Culture |
New Culture |
|
Attitudes to Dementia Care |
|
|
Paternalistic attitude Cared for in asylums Little reward |
Positive attitude Proactive in care High rewards |
|
General View of Dementia |
|
|
Dementia as neurological impairment |
Dementia as disability |
|
Ultimate Source of Knowledge |
|
|
The doctors and brain specialists know best |
The skilled and insightful practitioners of care know best |
|
Emphasis for Research |
|
|
We have to wait until we find the biomedical breakthrough |
We have to work now on improving skills and gaining insight |
|
Us and Them |
|
|
People with dementia are significantly different from those who do not have dementia |
People with dementia are the same as anyone else and should be treated as such |
|
What Caring Involves |
|
|
Focus is on what is obvious and easily managed (i.e. meeting basic needs and keeping them safe) |
Focus is on personhood, and this involves more than simply meeting basic needs and safety issues |
|
Priorities for Understanding |
|
|
Extent of impairments and deficits and relate this to stage of decline |
Extent of remaining abilities and resources |
|
Problem Behaviours |
|
|
Emphasis is on controlling the behaviours |
Emphasis is on understanding meaning behind the behaviours |
|
Carer’s Feelings |
|
|
Set aside our own feelings and get on with the job in hand |
To be in touch with our own feelings and transform these into positive resources for our work |
|
Personhood of Staff |
|
|
They are servants of the organisation |
They are people who should be just as respected as the patients they work with |
Some of these aspects of the culture of care have been discussed in earlier units (for example, the general view of dementia in Unit Two) and some will be discussed in later units (for example, problem behaviours in Unit Four). Kitwood (1995:11) summarises the differences between these two cultures by stating that:
“The old culture is one of alienation and estrangement. Through it we are distanced from our fellow human beings, deprived of our insight, cut off from our own vitality. The old culture is one of domination, technique, evasion and buck-passing. To enter the new culture is like coming home. We can now draw close to other human beings, accepting all that we genuinely share. We can recover confidence in our own power to know, to discover, to give, to create, to love. And this homecoming is a cause for joy and celebration”
By way of conclusion to this Unit, it would be useful for you to evaluate your current area of practice in light of what you have learnt in this Unit.
|
|
ACTIVITY 3.16: QUESTION |
Brooker (2007) proposes certain “indicators” that are helpful in evaluating your care in light of her VIPS model.
Consider your area of practice in light of these indicators and consider what evidence there is for any that you answer “Yes” to.
Valuing People
Is there a vision and mission statement about providing care that is person-centred? Yes/No
Evidence?
Are systems in place to ensure staff feel valued by their employers? Yes/No
Evidence?
Are there practices in place to support development of a workforce skilled in person-centred care? Yes/No
Evidence?
Individualised Care
Do you identify strengths and vulnerabilities across a wide range of needs and have individualised care plans that reflect a wide range of strengths and needs? Yes/No
Evidence?
Do service users have their own personal clothing and possessions for everyday use? Yes/No
Evidence?
Are individual likes and dislikes, preferences and daily routines known about by direct care staff and acted upon? Yes/No
Evidence?
Personal Perspective
On a day-to-day basis, are service users asked for their preferences, consent and opinions? Yes/No
Evidence?
Do staff show the ability to put themselves in the position of the person they are caring for and to think about decisions from their point of view? Yes/No
Evidence?
Is the physical environment (eg noise, temperature, etc) managed on a day-to-day basis to help people with dementia feel at ease? Yes/No
Evidence?
Social Environment
Are people with dementia helped by staff to be included in conversations and helped to relate to others? Is there an absence of people being “talked across”? Yes/No
Evidence?
Are people’s fears taken seriously? Are people left alone for long periods in emotional distress? Yes/No
Evidence?
Do staff help people with cognitive difficulties to be active in their own care and activity? Is there an absence of people being treated like objects with no feelings? Yes/No
Evidence?
|
|
Unit Summary |
This unit has considered the nature of care in relation to working with people with dementia. It has discussed what constitutes care, the nature of person-centred care, and the need to consider the central importance of the relationship. It has also highlighted the need to consider the organisational context within which care occurs. All of these will have an impact on the quality of care that the person with dementia and their families will receive, and will also have an impact on the professional carers working within these organisational structures.
To conclude, here are the words of a person with dementia:
“How you relate to us has a big impact on the course of the disease. You can restore our personhood, and give us a sense of being needed and valued. There is a Zulu saying that is very true. “A person is a person through others”. Give us reassurance, hugs, support, a meaning in life. Value us for what we can still do and be, and make sure we retain social networks. It is very hard for us to be who we once were, so let us be who we are now and realise the effort we are making to function.” (Bryden, 2005: 127)
|
|
Further Reading |
Baldwin C (2008) Toward a person-centred ethic in dementia care: doing right or being good? In: Downs M and Bowers B (eds) Excellence in Dementia Care: Research into practice Open University Press: Maidenhead
Brooker D (2007) Person-Centred Care: Making services better Jessica Kingsley Press: London
Kitwood T (1997) Dementia Reconsidered: the person comes first Open University Press: Buckingham
|
|
References |
Baldwin C (2008) Toward a person-centred ethic in dementia care: doing right or being good? In: Downs M and Bowers B (eds) Excellence in Dementia Care: Research into practice Open University Press: Maidenhead
Beach MC, Inui T and the Relationship-Centred Care
Research Network (2006) Relationship centred care: a constructive
reframing Journal of General Internal
Medicine 21(S1): S3-S8 [online:]
http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=1484841&blobtype=pdf
(accessed: 03-03-09)
Brooker D (2004) What is person-centred care for people with dementia? Reviews in Clinical Gerontology 13(3): 215-222
Brooker D (2007) Person-Centred Care: Making services better Jessica Kingsley Press: London
Bryden C (2005) Dancing with Dementia: my story of living positively with dementia Jessica Kingsley Press: London
Cassel EJ (1982) The nature of suffering The New England Journal of Medicine 306: 639-645
Cox S (1998) Housing and Support for People with Dementia HACT: London
Cox S (2001) Developing quality in service In: Cantley C (ed) Handbook of Dementia Care Open University Press: Buckingham
Dennis M and Morgan L (2008) Leading a dignified revolution Nursing Management 15(8): 14-15
http://dignifiedrevolution.org.uk/documents/Leading a Dignified Revolution 0812 article.pdf
Department
of Health (2001) National Service
Framework for Older People [online:]
http://www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/DH_4003066
(accessed: 29-09-08)
Department of Health (2003) Single Assessment Process for Older People: the accreditation process for off-the-shelf assessment tools [online:]
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4070322 (accessed: 05-03-09)
Department of Health (2009) Living Well with Dementia: A National Dementia Strategy [online:] http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_094058 (accessed: 14-02-09)
Dworkin R (1993) Life’s Dominion: an argument about abortion, euthanasia, and individual freedom Vintage: New York
Gaster L (1995) Quality in Public Services: Managers’ Choices Open University Press: Buckingham
Kitwood T (1990) Concern for “Others”: a new psychology of conscience and morality Routledge: London
Kitwood T (1995) Cultures of care: tradition and change In: Kitwood T and Benson S (eds) The New Culture of Dementia Care Hawker: London
Kitwood T (1997) Dementia Reconsidered: the person comes first Open University Press: Buckingham (relevant chapter!)
Kuhn D and Verity J (2002) Putdowns and uplifts: signs of good or poor dementia care Journal of Dementia Care Sep/Oct: 26-28
Nolan MR, Davies S and Grant G (Eds) (2001) Working with older people and their families: Key issues in policy and practice Open University Press: Buckingham
Nolan MR, Davies S, Brown J, Keady J and Nolan J (2004) Beyond ‘personcentred’ care: A new vision for gerontological nursing International Journal of Older People Nursing 13(3a): 45–53
Suchman AL (2006) A new theoretical foundation for relationship-centred care Journal of General Internal Medicine 21(S1): S40-S44 [online:]
http://www3.interscience.wiley.com/cgi-bin/fulltext/118582936/PDFSTART (accessed: 22-02-09)
Whitehead A (1969) In Service of Old Age: the welfare of psychogeriatric patients Penguin: London
|
|
TUTOR TALK: Congratulations on coming to the end of this unit. Move on and answer the questions then return your completed test paper to the College for marking. Good luck and well done. |
© Copyright Reserved
Dementia
Awareness Certificate Course – Unit Three – Page